

Follicular Unit Excision

Follicular Unit Excision (FUE) has emerged as a highly effective method for harvesting donor hair follicles in Hair Restoration Surgery (HRS). It utilizes manual, motorized, or robotic devices to extract individual follicular units in situ without leaving a linear donor scar, unlike the classic Linear Strip Excision (LSE) technique. The FUE technique is particularly advantageous for patients desiring short hairstyles and hiding signs of surgery. Over the last two decades, the global demand for FUE has propelled the market size of HRS market to unprecedented levels.
FUE Technique: When applied correctly
While “lege artis” FUE has revolutionized HRS industry by offering excellent cosmesis, minimum downtime, and high patient satisfaction, its popularity is partly fueled by misconceptions, such as claims of being “minimally invasive,” “scarless,” or “not even surgery.”
Unfortunately, these notions are often perpetuated by illicit clinics that offer low-cost FUE procedures performed by inexperienced technicians on unsuspected patients.
Risks and pitfalls of the FUE technique
The FUE technique appears deceptively uncomplicated and has attracted myriads of neophyte surgeons who falsely believe that the learning curve of FUE is short just because the barrier of entry is low, and no previous surgical skill is required.
The appeal of FUE comes with inherent challenges, including the extremely high potential for graft injuries (since it is a blind technique) and long-term irreversible side effects if not performed properly.
Απαιτήσεις και εκπαίδευση για την τεχνική μεταμόσχευσης μαλλιών FUE
Surgeons undertaking FUE must possess a comprehensive understanding of the nuances of the technique to ensure consistent graft quality and favorable cosmesis in both donor and recipient areas. Achieving proficiency in FUE necessitates scientific knowledge, lengthy training, dexterity, enthusiasm, cognitive clarity, experience, and dedication to the required prolonged learning curve.
While FUE stands as a valuable addition to the armamentarium of an HRS surgeon, its judicious application is paramount. This article delves into the evolution, challenges, and critical aspects of skillful FUE implementation in the field of HRS.
KEY WORDS:
FUE technique, donor harvest, scarless, graft transection, FUE megasession, donor area depletion, overharvesting, graft injury, manual punch, motor-FUE, manual-FUE, surgery delegation
HAIR TRANSPLANTATION: HISTORY & EVOLUTION
Hair Restoration Surgery (HRS) has weathered a tumultuous history, bearing the weight of a questionable reputation for decades. Dating back to the 1960s, the results of earlier techniques and the misuse of more contemporary approaches have left an indelible mark on countless patients, leading to the stigmatization of HRS within both the medical community and the public perception.

Failed techniques and big mistakes of the past
Regrettably, the past of HRS is marked by instances of poor surgical judgment, thoughtlessness, and a steadfast adherence to outdated practices.
The repercussions of these mistakes have been profound, with the acquisition of knowledge through experience proving to be a slow and arduous process. However, amid the shadows of controversy, a cadre of ambitious and ethical surgeons has risen to question the entrenched “dogmas” of earlier HRS techniques. These pioneers embarked on experimental journeys aimed at achieving natural results and surmounting surgical challenges. Their dedication to advancing the scientific foundation of HRS led to the dismantling of older, obsolete, and illogical techniques that had plagued the field for decades.
The FUT technique as a milestone.
The consequences of these “mistakes” were profound, with the acquisition of knowledge through experience proving to be a slow and difficult undertaking. The Linear Strip Excision (LSE) technique, or FUT Hair Transplantation, marked the beginning of the end for those irrational and destructive hair implantation methods.
This technique was based on extracting follicular units in a single strip through an elliptical section of the scalp, suturing the donor area, and subsequently dissecting it into smaller grafts—elements that have remained as a legacy in modern hair transplantation.
Ethical Surgery & Scientific Progress
Thus, after three decades of dogmatism and “head-in-the-sand” attitudes, a group of ambitious and ethical surgeons revisited the “axioms” of the past and, through observation and the sharing of experience, began laying the foundations for evidence-based practices, with progressively less tissue damage and more natural results.
Their dedication to advancing the scientific basis of hair transplantation led to the collapse of the outdated, irrational techniques that had plagued the field for decades.
The discovery of the FUE technique – A new era
The quest for graft extraction without the “cosmetic cost” of a linear scar emerged as a new frontier, prompting pioneering surgeons to tackle this challenge. With careful surgical technique, in FUT Hair Transplantation, the donor area heals leaving an almost imperceptible scar, only 1 mm in width, which is easily concealed by hair as short as half a centimetre.
However, the very existence of an incision and sutures caused hesitation among patients. Thus, the need arose for an alternative method of hair excision and follicular unit transplantation.
FUE: The technique that changed hair transplantation
The method discovered and published in 2002 by Bernstein & Rassman involved extracting follicular units (FUs) one by one using tiny cylindrical instruments (punches) instead of a scalpel.
The technique discovered by Bernstein & Rassman was named Follicular Unit Excision (FUE).
The only difference between the FUE technique and the FUT technique lies in the method of extracting the follicular units from the donor area, as all the other steps of the procedure are the same.
The FUE technique today: Innovation and competition
This innovation was the starting point for a competitive race among surgeons, who sought technical excellence in FUE, constantly advancing with improvements, new instruments, and greater precision in performing hair transplantation with the FUE technique.
FUE became an evolutionary force in response to the growing demand for improved appearance and patients’ desire to avoid the donor area scar left by the FUT method.
Today, FUE hair transplantation is regarded as a modern, advanced surgical procedure with minimal scarring, steadily gaining ground thanks to its results and the natural hair density it provides.
The Popularity of FUE: Smaller Scars and More Candidates for Hair Transplantation
The primary motivation behind employing FUE lies in its ability to circumvent the creation of a visible linear scar, thereby allowing patients the flexibility to wear their hair short. Beyond this fundamental advantage, patients were assured of several side benefits, including:
- markedly reduced post-operative discomfort or pain
- expedited surgical recovery
- minimal disruption to an active professional, personal, or social lifestyle
- an increase in scalp donor capacity (enabling safe harvesting from areas superior and more anterior to the ears and the nape of the neck)
- diminished limitations imposed by scalp laxity, and
- the prospect of expanding the potential donor area to include body hair.
Who is the FUE Hair Transplantation Technique for?
Furthermore, FUE proved to be particularly advantageous for specific patient demographics:
- Young patients, who are inherently at a higher risk for developing wider scars after LSE, can undergo FUE without such concerns
- Individuals with limited areas of alopecia other than androgenetic alopecia (AGA)
- Individuals with previous LSE surgeries seeking to camouflage older scars by implanting FUs inside the existing scar without removing it and
- Patients with a history of wide scars or hyper-elastic skin
- Patients with scars from various causes, including dermatologic conditions (scarring alopecias), trauma, or neurosurgical procedures
- Individuals who are apprehensive about the incision and sutures involved in the FUT technique
- Individuals with a history of highly active scarring (keloids) or collagen disorders (Ehlers-Danlos syndrome): in these rare cases, the FUE technique may be used with a lower (though still present) risk of complications
- Individuals whose scalp donor area has been completely depleted and who require the use of FUs from alternative body areas, through the Body Hair Transplant (BHT) technique.
The versatility of FUE not only addresses the aesthetic concerns of patients but also extends its applicability to diverse clinical scenarios, making it a valuable and multifaceted tool in the realm of HRS.
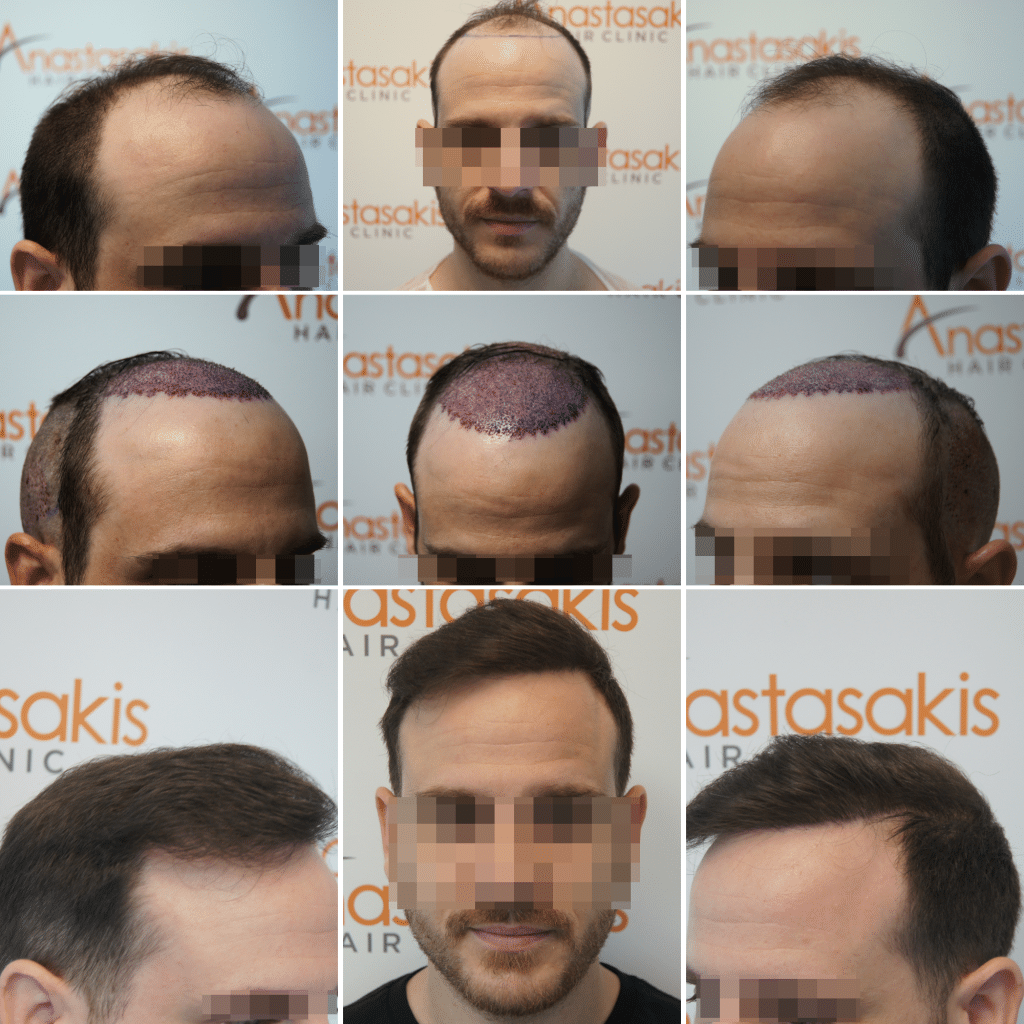
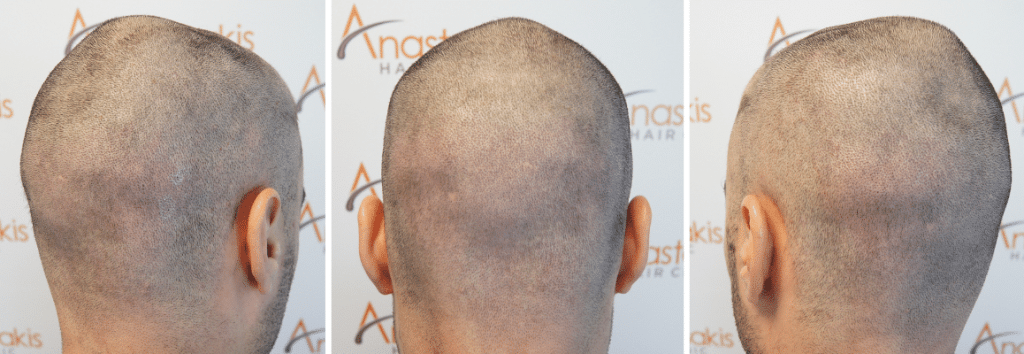
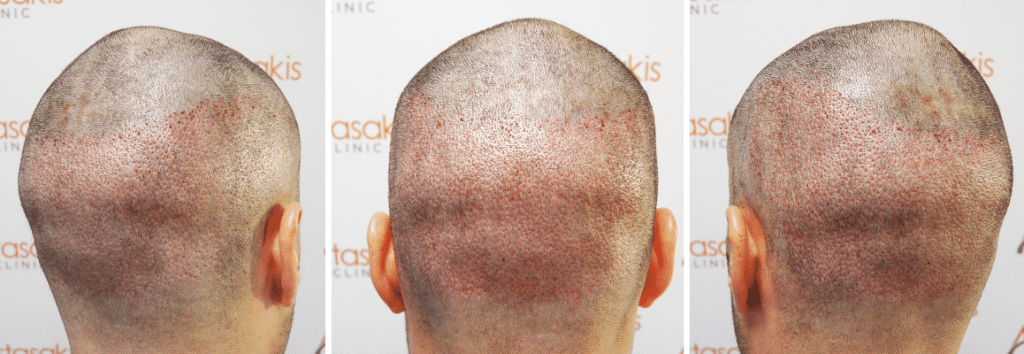
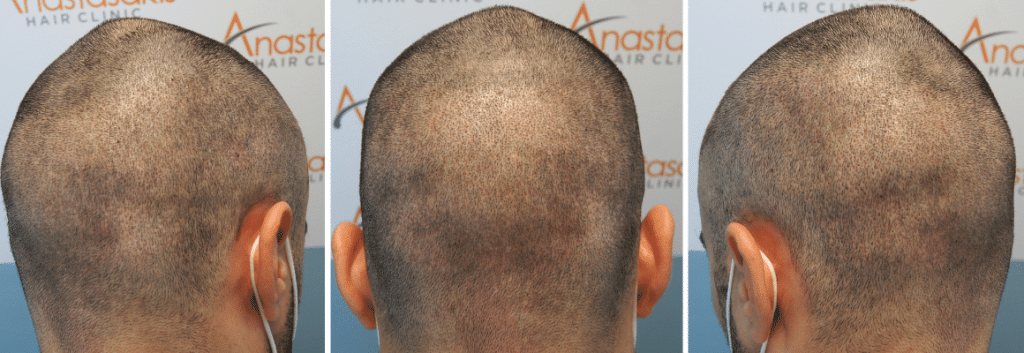
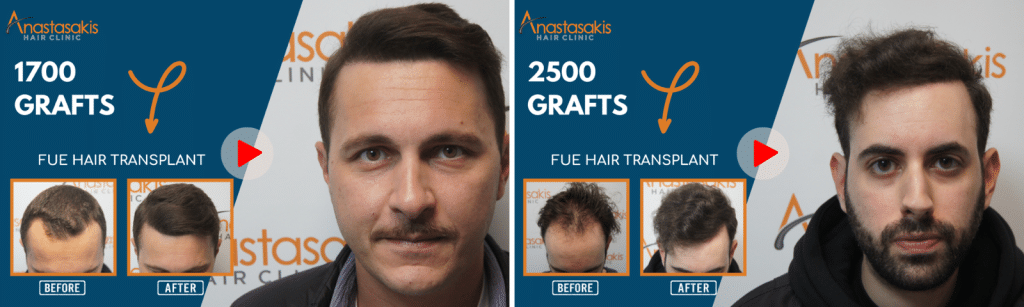
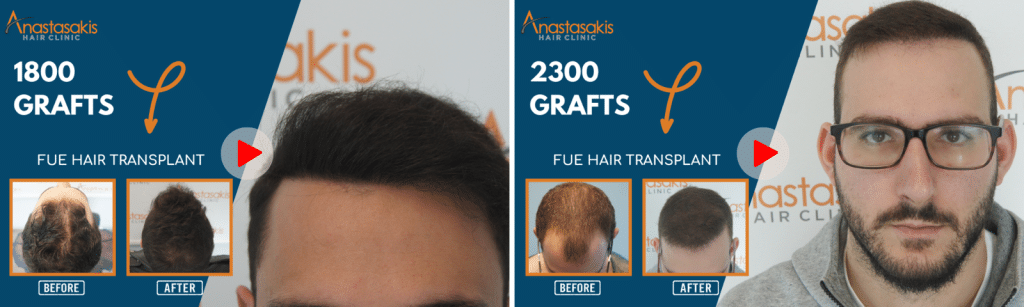
See Before-and-After Results of FUE Hair Transplantation at Anastasakis Hair Clinic.
FUE Hair Transplantation – A Scar-Free Technique
To dispel a common misconception influenced by enthusiasm and deceptive advertising, it is crucial to recognize that FUE is not a scarless technique but rather a scar-spreading technique. To be precise, the ISHRS prohibits its members from using in their informational brochures or advertising messages terms such as: ‘scar-free procedure’ (‘No scars’), ‘incision-free procedure’ (‘No incision’), ‘no-touch procedure’ (‘No touch’), ‘cut-free procedure’ (‘No cutting’), and ‘non-invasive procedure’ (‘Non-invasive’).

The ISHRS explicitly prohibits its members from including terms such as the following in informational brochures or promotional materials:
- «No scars session»
- «No incision session»
- «No touch session»
- «No cutting session»
- «Non-invasive session».
Scar tissue does exist, it is simply not so visible to the naked eye unless the hair is cut very short. The reason it is not apparent lies in the construction of the human eye, not in the FUE technique itself! The human eye can detect and follow a straight line thinner than a hair, but it cannot ‘distinguish’ the thousands of 1 mm circular scars among the hair.
Advantages of the FUE Technique for Patients
- If FUE is executed “lege artis”, the patient can maintain a very short hairstyle even after extensive harvesting and several FUE sessions
- No stitches are required, the donor area heals within 7–10 days, and no additional visit is needed for suture removal
- Post-operative discomfort is minimal; post-surgical painkillers are rarely required
- Surgical recovery is rapid, with incisions typically healing in just 3-5 days. This leads to minimal downtime and easily concealable wounds.
- Patients with active lifestyles face no significant exercise restrictions, allowing them to resume standard simple activities even on the next day and heavy training in a week
- Scalp laxity limitations and issues arising from multiple previous donor area scars of any source are practically nonexistent
- Complications related to nerve and vessel injuries are exceedingly rare, although reports of widespread anagen effluvium in the donor area exist when harvesting is extremely extensive or inappropriate tools are used
- Patients with advanced AGA may undergo two or three consecutive FUE sessions on consecutive days to cover their cosmetic goals sooner
- FUs from various body areas, such as the beard, chest, abdomen, back, hands, legs, and genitals, can be successfully transplanted. (Body Hair Transplant)
Watch FUE Hair Transplant Results in Videos from Anastasakis Hair Clinic.
Disadvantages of the FUE Technique for Patients
- The primary drawback is the reduction of total donor capacity when exclusively utilizing the FUE technique, which limits the number of grafts safely harvested over one session and one’s lifetime. Of course, the proper combination of the FUE and the FUT technique, or the use of Body Hair FUE, solves this problem.
- When the FUE technique is performed by untrained or non-medical personnel, follicular damage and the high transection rate of follicular units are extremely elevated. When follicles are destroyed during extraction, the final survival rate is reduced, leading to a lower number of hairs ultimately growing in the recipient area
- The FUE procedure is prolonged compared to an LSE session, leading to patient fatigue
- Daily graft extraction is limited, necessitating multiple sessions over 2 or 3 days, or 6-12 months after the previous harvest
- Higher cost per graft in FUE
- Complete shaving of the entire donor area to 1-2mm (total shave) is required in FUE, is associated with social discomfort. However, the rising popularity of long-hair FUE addresses this concern among patients and surgeons
- Women will not agree to shave the donor area to help the surgeon identify hair follicles and their exit angle when performing FUE
- Extensive microscopic devascularization injury in the donor area may lead to permanent “thin” areas. This can occur after multiple FUE sessions or a single injudicious harvest
- Very curly/coily hair with a powerful “character” beneath the skin carries an increased risk of graft transection in FUE.
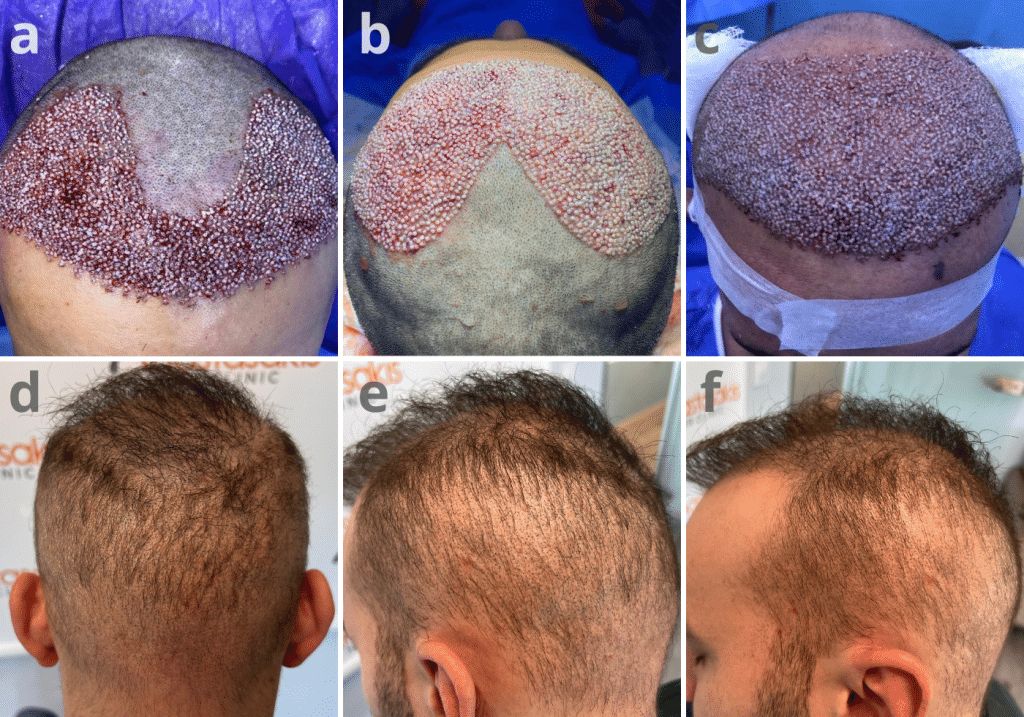
How the FUE Hair Transplantation Technique Is Performed?
FUE hair transplantation is performed in two basic steps:
- Excision of the follicular unit (FU) from the scalp (follicular isolation) using specialised instruments.
- Collection/extraction of the follicular unit (follicular excision – collection) using forceps.

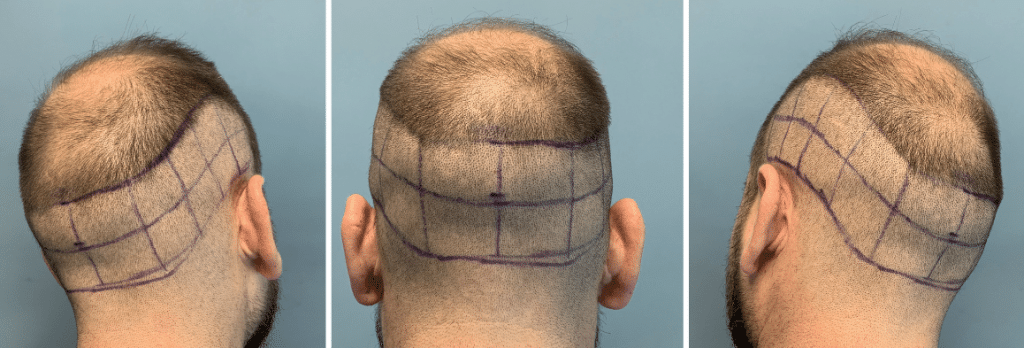
Donor Area Characteristics
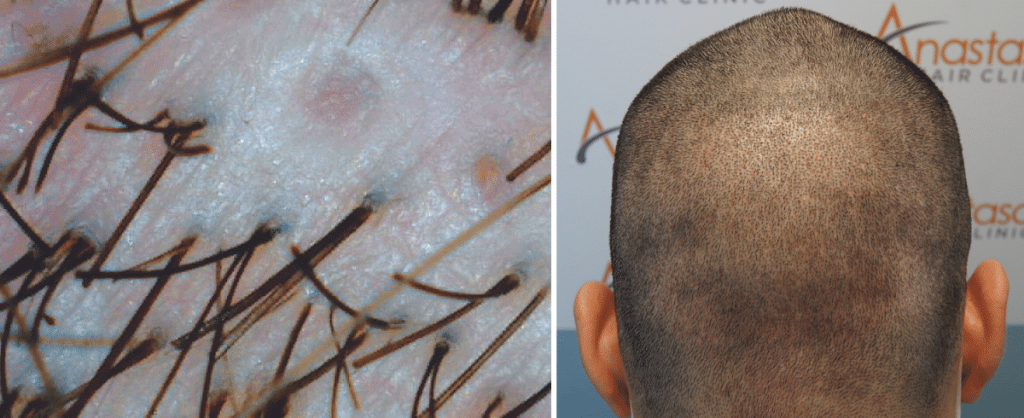
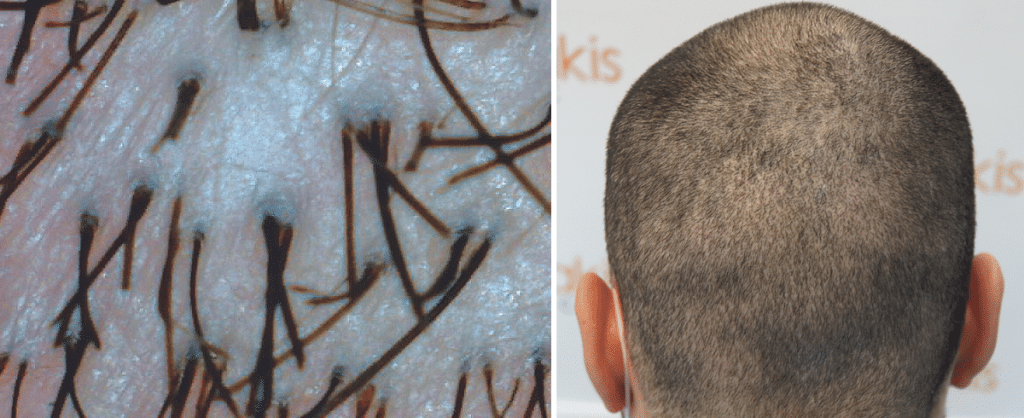
The tiny cylindrical incisions from the follicular units removed from the donor area heal without suturing.
These incisions are covered by the remaining hair and are almost imperceptible, even when the hair is only half a centimetre long, provided that overharvesting in the donor area is avoided.
FUE vs FUT: The Key Difference
All other technical details and procedural steps in hair transplantation with the FUE technique are identical to those of the FUT technique.
The difference between the two modern techniques, FUE and FUT, lies solely in the method of graft extraction from the donor area.
Application of the FUE Technique at Anastasakis Hair Clinic
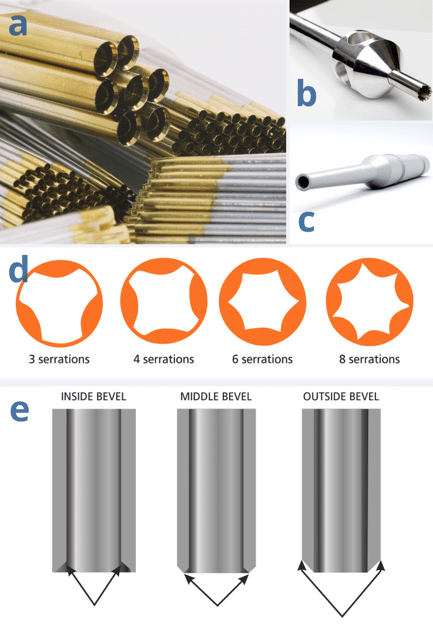
At Anastasakis Hair Clinic, hair transplantation with FUE is performed with:
- Extraction of follicular units one by one from the donor area, using FUE titanium manual punches or
- Mechanical MAMBA punches (Trivellini ‘flared’ and ‘edge-out’)
- Alternatively, blunt punches are used (Harris S.A.F.E™ hexagonal punch).
The Extraction of Follicular Units in the FUE Technique
The rationale behind FUE involves employing a circular punch to excise a tissue column comprising an intact FU along with all layers of the skin
“Intact” is the key term; the surgeon must exert every effort to prevent any trauma to the harvested hair follicles, with transection or amputation representing the most severe forms of injury.

The extremely delicate nature of the FU renders it susceptible to various forms of harm during the harvesting process, giving rise to a multitude of challenges inherent in extracting individual FUs with tiny punches while avoiding follicular transection or amputation
Fundamental Steps in Successful FUE Extraction
In summary, the successful extraction of FUE grafts involves specific universal steps:
- Targeting
- Incision / Scoring
- Extraction
- Collection
Evolution and Refinements of the FUE Technique
The collaborative endeavors of a handful of surgeons have substantially enhanced the techniques, technologies, and tools associated with FUE, resulting in a noteworthy improvement in service quality and results since 2002.
Presently, employing various available FUE approaches, practically all patients can undergo successful harvesting, marking a significant achievement.
Why Shaving of the Donor Area Is Required in the FUE Technique?
In order to perform FUE harvesting under proper conditions, the entire donor area must be shaved down to 1mm (total shave).
For most patients, the considerable benefits of FUE more than offset the social problems seen with the shaved donor area, which have to be managed for the first week or so after an FUE procedure.
There is a demographic of HRS candidates who, for professional, social, or personal reasons, are highly self-conscious of their appearance and do not consider that the benefits of FUE will counterbalance the social awkwardness of a fully shaved donor area.
Older male patients who typically have no intention to ever buzz-cut their hair might also be included in this group, and therefore, the cosmetic “freedom” that FUE offers is irrelevant to them. Others are reluctant to trim their hair because scars from previous LSE operations will show.
Alternative Techniques of Shaving and Follicular Unit Isolation
Solutions to bypass these issues have been offered. These include partial-shaving “tunnels” (microstrip shaving) along the back and sides of the head, each 2 to 3 cm wide, leaving the overlying longer hairs to conceal the trimmed hairs.
Another idea is an individual follicular trim isolation technique, trimming only those hairs that will be extracted. These techniques are very time-consuming, and unless the surgeon is highly experienced, harvested areas may be left with significant thinning.
These techniques also risk creating a so-called “zebra effect” or “flag-sign” scarring due to horizontal rows of the scalp that are thinned out from FU harvesting, which is cosmetically worse than a strip scar. Recently, long-hair FUE has been suggested to by-pass all these issues, but a small number of grafts can be extracted safely per day.
Shaving of the donor area in FUE remains the safest and most efficient protocol for extracting a large number of grafts, while alternative methods have a role in specific cases and require careful planning by specialised surgeons.
Body Hair-to-Scalp FUE (BHT)
FUE allowed for the first time to easily harvest body hair follicles and use them in HRS. Body-to-Scalp Hair Transplantation (BHT) involves the harvesting of FUs from areas other than the scalp and their transplantation into the scalp or other hairy areas.
Of course, beard and other body donor hair differ in characteristics (maximum length, caliber, color, growth cycles, etc.) from the scalp donor hair since they are typically shorter, single-haired, thinner, and less “shiny” compared to scalp hair.
Surprisingly, when these FUs are transplanted to the scalp, they gradually show an ability to reshape their morphology and iteratively converge to the recipient tissue environment by significantly prolonging anagen duration, eventually growing much longer than earlier.
When Is Body Hair Transplant Applied?
Combining or “mixing” BHT FUs with scalp donor FUs on selected individuals was initially presented as a “miracle solution” that could increase the number of potentially transplantable FUs enormously and expand the candidate pool to cases that were previously deemed inoperable.
When the initial enthusiasm was subdued through bitter experience, graft harvesting in BHT proved to be very challenging, having a very long learning curve, with characteristically high follicular transection rates, and often disappointing post-operative graft survival. Especially when non-beard BHT grafts are harvested, the donor area heals slower, and local complications are more frequent than in the scalp.
Notably, only highly trained FUE experts will successfully employ BHT, and not even those may claim that the results on the recipient area are consistent and predictable.
Most experts consider BHT as an ultimate, “last resort” solution that should be applied under specific, unique circumstances and for the following indications:
- Cases with extremely unfavorable donor-to-recipient needs ratio. Low donor reserves can be attributed to low donor density, narrow donor fringe, retrograde alopecia, previous surgical or post-traumatic scarring, extensive donor miniaturization, diffuse thinning, and very fine, straight hair. High recipient needs can result from big skull size, advanced AGA, early age of onset, rapid progression of AGA, low-residual hairline, and high hair-to-scalp color contrast. In all these cases, however, the surgeon should first follow established guidelines/protocols on scalp donor area harvesting. The surgeon should not rely on BHT grafts to “save the day”.
- Camouflage of scalp scars, from previous LSE surgery, punch grafts, flaps, burns, or other injuries for which the patient is unwilling to use “precious” scalp FUs or when the scalp donor area is naturally poor or depleted due to previous surgery.
- Combining or “mixing” beard FUs with scalp donor FUs to improve recipient area density and/or the cosmetic result in individuals with depleted/overharvested scalp donor area. “Combination grafting” of scalp-plus-beard hair not only increases the total number of donor hair but enhances results because of the larger diameter and coverage value of beard hair.
- Use of thin body hair follicles in areas where hair thickness, growth rate, and length desired are optimal for body hair but not for scalp hair. These include areas where a “thin look” is preferable, such as feathering the hairline , use on the temple points, or the reconstruction of eyelashes, eyebrows, etc.
- To reconstruct small areas of beard in Zones 1-3, which are necessary for secondary sexual male characteristics. In that case, one can recycle beard hair from other, less important beard areas. (Fig. 13)
Overall, the experience gathered in BHT has been substantial since the late 2000s. It clearly has a place in modern HRS on many occasions but is performed at an acceptable standard by only very experienced surgeons.
Female Alopecia and Hair Transplantation with the FUE Technique
Women with any alopecia that is eligible for HRS, most often FPHL or scarring alopecia, will rarely, if ever, agree to entirely shave the donor area to help the surgeon identify hair follicles and their exit angle when performing FUE.
This understandable unwillingness to shave the donor area makes FUE megasessions practically impossible for these female patients. Therefore, the size of an FUE session in these women is limited to techniques such as:
- Microstrip shave
- Camouflage-to-go
which will offer a smaller number of FUs compared to a full FUE session.
Therefore, LSE surgery is typically preferred in women. However, one should remember that in most women with FPHL, the donor area often presents a high ratio of miniaturized hair follicles. In these cases, the surgical advantage of cherry-picking “healthier” grafts with FUE can be a determining factor in the final result and should be explained to these specific female candidates.
The Challenges in the Application of the FUE Method
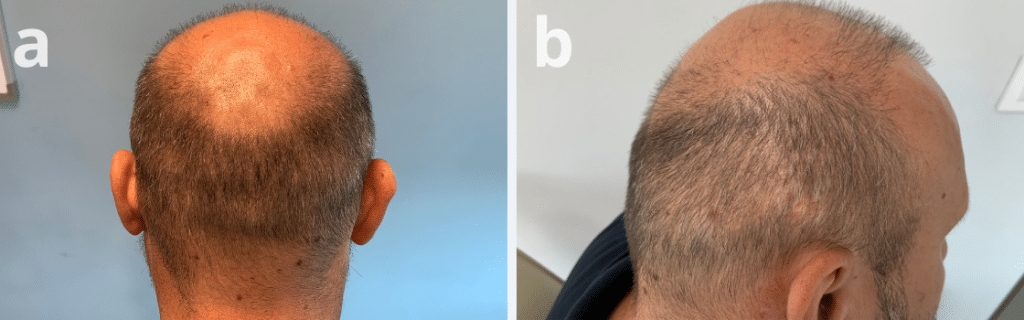
Overharvesting
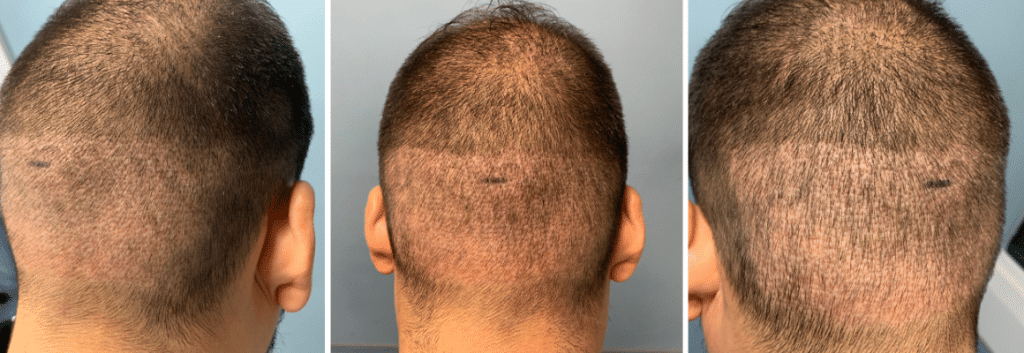
Unfortunately, the global surge in FUE popularity has led to a massive rise in cases of donor area overharvesting, resulting in severe cosmetic defects ranging from visibly moth-eaten donor areas to near-complete donor alopecia.

Evaluating the permissible number of harvested grafts and surgical trauma in FUE before reaching a noticeable decrease in coverage remains an ongoing challenge. No single algorithm comprehensively integrates all the various factors to predict the minimum adequate remaining donor area density following FUE.
Therefore, surgical experience and prudent harvesting are paramount. To predict FUE harvest limits and prevent overharvesting, some FUE experts propose guidelines based on the initial “Hair Coverage Value” derived from hair shaft diameters and hair count/cm2. However, no metric or index can substitute for clinical judgment and thoughtful consideration
Hair Follicle Trauma in the FUE Technique
The incidence of injuries to FUE grafts is variable and strongly influenced by the surgeon’s skills. Follicular transection stands out as a prevalent form of injury associated with FUE.
Minimizing the transection and injury rates primarily relies on the surgeon’s:
- expertise
- encompassing experience
- eyesight
- hand-eye coordination, and
- maneuvering capabilities.
Mega Sessions FUE
In recent times, FUE megasessions are being touted as contemporary alternatives to LSE megasessions. Advances in technology, improved punch designs, enhanced training, and accumulated experience, have enabled surgeons to push the boundaries of FUE megasessions well beyond 1500 FUs in a day.
The greatest risk is when an FUE megasession is poorly performed leads to decimated, see-through, moth-eaten, and thin donor areas. This is a characteristic outcome associated with unsupervised indifferent operators, often anonymous technicians operating on unsuspecting patients in low-cost FUE destinations.
How to Choose the Right Clinic and Surgeon for FUE Hair Transplant
In an unregulated FUE landscape, the field of HRS is encountering a growing threat to its reputation due to the escalating prevalence of suboptimal outcomes delivered by unlicensed practitioners. These practitioners often operate on unsuitable surgical candidates, make unrealistic promises, engage in overharvesting of donor areas, and create unnatural hairlines. It is tragic to put the beautiful FUE results produced by skilled HRS surgeons side-by-side with the disfiguring results of these “money mills”.
Consider the following factors when selecting a hair clinic or surgeon for your FUE hair transplant:
AUTHORITY – Doctor’s credentials, experience and knowledge
- Doctor’s Training and Experience: Before entrusting your FUE hair transplant to any clinic, it’s imperative to thoroughly assess the doctor’s training and experience. Dr. Konstantinos Anastasakis, the Medical Director of Anastasakis Hair Clinic, boasts an impressive background with an MD, PhD, and affiliations with prestigious organizations like ISHRS (International Society of Hair Restoration Surgery) and ABHRS (American Board of Hair Restoration Surgery). This ensures that you are in the hands of a highly qualified and experienced professional.
- International Recognition: International recognition is a strong criterion for selecting a hair loss clinic. Dr. Anastasakis and Anastasakis Hair Clinic are affiliated with renowned organizations like ISHRS and ABHRS, reinforcing their commitment to excellence on a global scale.
SAFETY – Doctor’s credentials, experience and knowledge
- Location and Licensing: Anastasakis Hair Clinic operates in accordance with the law, with medical premises licensed to provide hair transplant services. When considering clinics, pay attention to the choice of location and the legitimacy of the medical facilities. Additionally, don’t be afraid to explore clinics beyond your city or even in another country, as the quality of results is often worth the investment in travel and accommodation
- Patient-Doctor Relationship: The success of your FUE hair transplant also depends on the relationship you establish with your doctor. Anastasakis Hair Clinic emphasizes the importance of feeling comfortable with your physician. Dr. Anastasakis is known for attentive listening, thorough answers to all questions, and a willingness to discuss various treatment options. A compatible patient-doctor relationship is crucial for a successful and satisfying hair transplant experience.
RESULTS – Videos of patients
- Remember to Request Before and After Result Videos: Anastasakis Hair Clinic encourages prospective patients to request before and after result videos as the most accurate way to assess a clinic’s track record. The clinic has a consistent history of successful hair restoration procedures, and these videos serve as tangible proof of the expertise and dedication to delivering natural and dense results.
Watch FUE Hair Transplant Results on VIDEO by Anastasakis Hair Clinic.
Why Choose Anastasakis Hair Clinic for your FUE Hair Transplant
At Anastasakis Hair Clinic, we pride ourselves on implementing specific procedures and maintaining excellent teamwork. Dr. Konstantinos Anastasakis’s extensive credentials, including being an ISHRS fellow member and a Diplomate & Board of Directors member to the ABHRS, underscore our commitment to technical excellence in FUE Hair Transplant.
Transparency and Proof of Our Exceptional Results
In addition to our esteemed credentials, Anastasakis Hair Clinic sets itself apart by providing unparalleled transparency and proof of our exceptional results. Unlike any other clinic globally, we have amassed hundreds of videos featuring real patients who have graciously shared their experiences and showcased their transformative results. These videos serve as tangible evidence of our clinic’s dedication to delivering natural and satisfying outcomes. When you choose Anastasakis Hair Clinic for your FUE Hair Transplant, you can trust that you’re not only in the hands of highly qualified professionals but also joining a community of satisfied patients whose lives have been positively impacted by our services.
Conclusion
In transforming the Hair Restoration Surgery (HRS) landscape, Follicular Unit Excision (FUE) has ushered in a new era marked by continual advancements in techniques and tools, enabling dedicated surgeons to consistently achieve excellent outcomes.
FUE demands a mastery that evolves over years, mandating a unique combination of dexterity, training, dedication, enthusiasm, cognitive clarity, scientific knowledge, and experience. It is imperative to recognize that FUE is a surgical procedure, and its practice should be confined to licensed physicians extensively trained in the technical and aesthetic facets of HRS. Properly executed, the aesthetic benefits and heightened patient satisfaction offered by FUE are undeniable.
Personal Assessment for Your Hair Transplant – Start today
At Anastasakis Hair Clinic, we are committed to delivering these outstanding results by combining expertise, experience, and dedication in FUE hair transplantation. Contact us today and take the first step toward a new, improved appearance with the FUE hair transplant technique!
To determine which hair transplant technique is right for you, contact us for a personal consultation and evaluation appointment. Send us your photos along with some basic information and your goals using the free hair transplant design form, and we will provide you with an assessment, usually within 3 working days.