
Introduction to Alopecia
Alopecia refers to any type of hair loss resulting from disease, dysfunction, autoimmune disorder, or hereditary predisposition. There are several types of alopecia, affecting both men and women, and each type of hair loss may have different underlying causes. Some forms are common, while others are rare or associated with autoimmune conditions or scarring alopecia.
Approximately 97% of alopecia cases are non-scarring (non-cicatricial) and therefore reversible, meaning that healthy hair follicles are not permanently destroyed. The remaining 3% of cases typically involve scarring alopecia, where irreversible damage occurs to the hair follicle stem cells, leading to permanent hair loss and sometimes complete baldness.
Understanding the different types of alopecia and identifying the specific type early is crucial, as timely treatment can restore hair growth and prevent further thinning.
Different Types of Alopecia
- Androgenetic Alopecia
Androgenetic Alopecia (AGA) is by far the most common cause of hair loss in both men and women. The term “androgenetic” accurately reflects the dual origin of the condition—“andro-“ refers to the hormonal component, and “-genetic” to the hereditary factor involved in its pathogenesis.
Androgenetic Alopecia is defined as the progressive miniaturization of normal terminal hair follicles on the scalp under the influence of androgens. This process gradually transforms terminal follicles into intermediate and eventually vellus follicles, which produce short, thin, colorless, and barely visible hairs with a significantly reduced lifespan.
There are two main types of Androgenetic Alopecia: Male Androgenetic Alopecia (MAGA) and Female Androgenetic Alopecia (FAGA).
- Male Androgenetic Alopecia (MAGA)
Male Androgenetic Alopecia (MAGA / Male Pattern Baldness)
In approximately 98% of men who lose hair, the cause is Male Androgenetic Alopecia (MAGA). Only about 2% of male cases are due to temporary hair loss caused by illness, thyroid disease, severe infection, or medication, which are usually reversible once the underlying medical condition is treated.
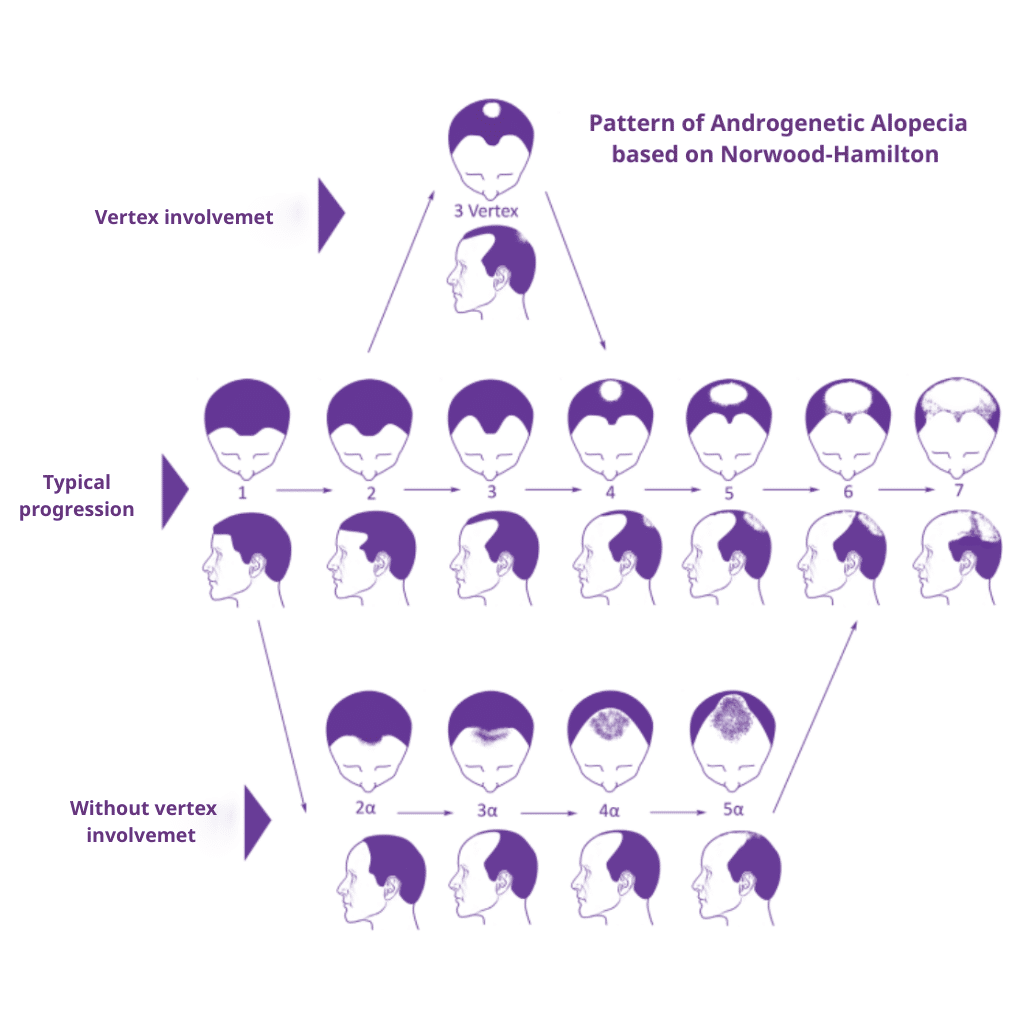
In men, male pattern baldness typically begins with a symmetrical recession of the frontal hairline at the temples, forming the classic “M-shaped” pattern hair loss. As the condition progresses, thinning
appears at the crown. Over time, these two areas may merge, leaving a strip of hair around the back and sides of the scalp.
Men who notice hair loss in their early twenties often experience it more extensively over time. In contrast, those who begin losing hair later in life may develop only partial alopecia or moderate hair thinning.
Each case of male pattern baldness is unique, and seeking an early male hair loss treatment plan is essential for slowing down its long-term progression.
While hair density naturally decreases with age, the pattern and rate of male hair loss vary widely. Some individuals may progress toward complete baldness, while others maintain much of their hair. Each case of male pattern baldness is unique and influenced by family history, hormonal levels, and genetic factors affecting the hair follicle’s sensitivity to dihydrotestosterone (DHT)
- Female Androgenetic Alopecia (FAGA)
Female Androgenetic Alopecia (FAGA) is the most common form of hair loss in women, and while it resembles male pattern baldness, it presents differently. Unlike men, women rarely develop complete hair loss or bald spots. Instead, they experience diffuse hair thinning over the top and crown of the scalp.
This type of alopecia can occur in women who are genetically predisposed, in those with hormonal imbalance such as androgen excess, or during menopause, when estrogen levels decline.
Only about 30% of women with FAGA show elevated androgenic hormones, indicating that most cases of female pattern hair loss are due to a combination of genetics, local hair follicle sensitivity, and age-related changes.
Women usually retain their frontal hairline, which distinguishes female pattern baldness from the male pattern. The main symptoms include thinning hair, reduced hair shaft diameter, and slower hair growth. In rare cases, frontal fibrosing alopecia, a subtype of scarring alopecia, can coexist and cause permanent hair loss along the hairline.
FAGA often develops in two peak age groups — during the 30s and around menopause (the 50s). Early-onset female pattern hair loss tends to progress more severely over time, while late-onset cases are usually milder.
Women affected by female pattern hair loss frequently report psychological stress, mental health concerns, and a negative impact on self-esteem, which underlines the importance of early diagnosis and starting an effective specialized female hair loss treatment early to preserve hair density and scalp health.

In contrast to men—where the onset of Androgenetic Alopecia typically peaks in the third and fourth decades of life—women tend to experience two peak periods for the onset of Female Androgenetic Alopecia (FAGA): the third and the fifth decade. The extent of FAGA is closely linked to the age of onset. Women who experience early-onset FAGA are more likely to develop more advanced stages of hair thinning over time. Conversely, those with late-onset FAGA rarely progress to the same degree of alopecia as seen in early-onset cases.

Alopecia Areata and Its Forms
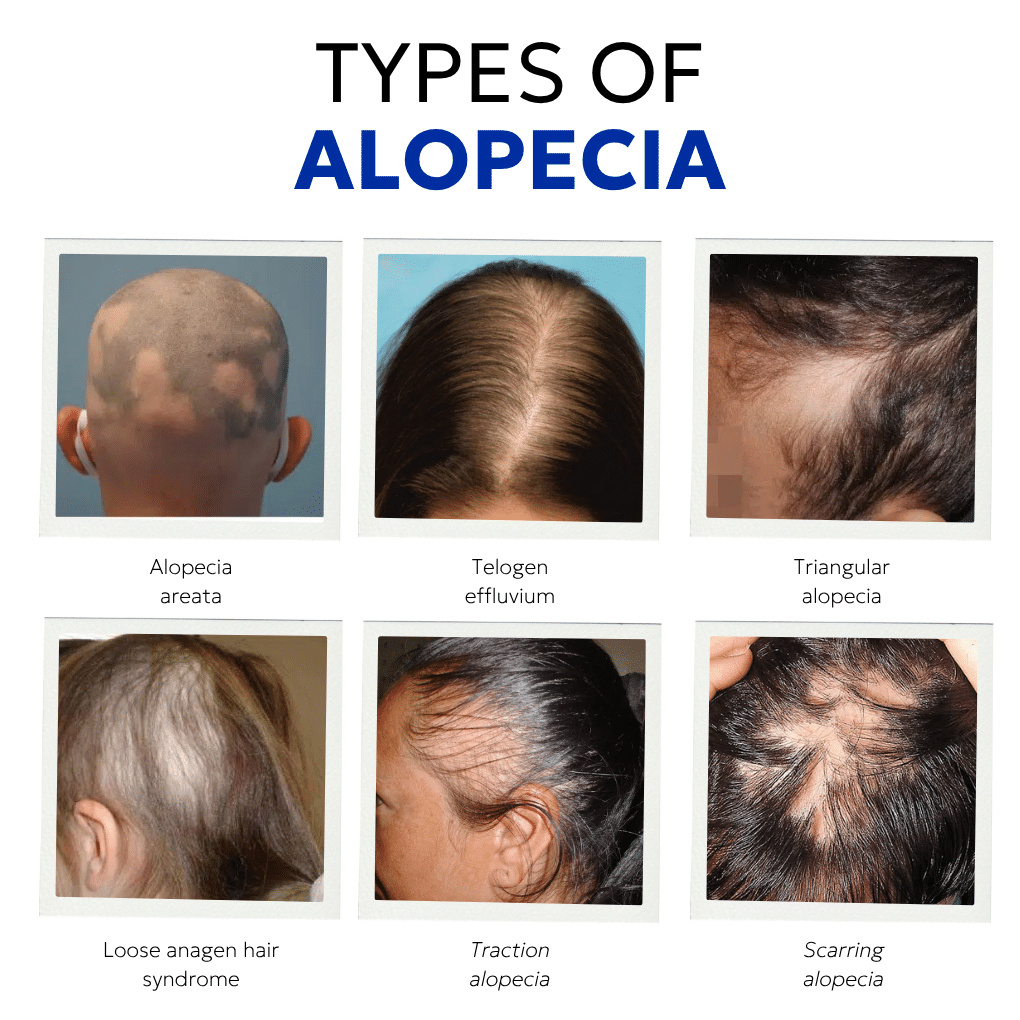
Alopecia Areata is an autoimmune disease in which the immune system attacks the hair follicles, leading to patchy hair loss on the scalp, beard (alopecia barbae), or other areas of body hair. It affects about 1–2% of the population and can occur in both men and women of any age.
Although the exact cause of alopecia areata remains unclear, it is believed to result from a combination of genetic susceptibility, immune system dysfunction, and environmental triggers. Stress, viral infections, trauma to the scalp, pregnancy, or thyroid disease may also contribute.
This condition is non-scarring and usually reversible, meaning the hair follicles remain structurally intact. In many cases, patients develop alopecia areata suddenly, noticing bald spots or circular patches.
Alopecia areata is not contagious, and the severity can vary from mild patchy alopecia areata to more extensive types.
Common Forms of Alopecia Areata
Because alopecia areata diagnosed cases vary widely, treatment options must be personalized. Early intervention often helps to grow hair again and prevent permanent hair loss.
- Patchy Alopecia Areata The most typical form, causing one or more bald spots with smooth skin. Hair regrowth may occur spontaneously or with treatment options like topical immunotherapy.
- Diffuse Alopecia Areata A less common subtype presenting as diffuse hair thinning across the entire scalp rather than distinct patches. It can resemble telogen effluvium or female pattern hair loss but is immune-mediated.
- Alopecia Totalis In this form, the patient experiences complete hair loss on the scalp, including eyebrows and eyelashes. It represents an advanced stage of alopecia areata.
- Alopecia Universalis This is the most severe form, resulting in complete hair loss over the entire body, including facial hair, eyebrows, and body hair. Like other types, it stems from an autoimmune condition.
- Ophiasis Pattern A subtype where hair loss appears in a band-like shape around the sides and back of the scalp, stretching from ear to ear. This form can be difficult to treat and may lead to further hair loss if not managed early.

- Telogen effluvium is a temporary hair loss condition, classified as non-scarring alopecia. Under normal circumstances, about 90% of scalp hair follicles are in the anagen (growth) phase and 10% in the telogen (resting) phase. In telogen effluvium, an abnormal number of hairs — sometimes more than 20% — enter the resting phase prematurely, causing noticeable thinning hair or shedding.Triggers include acute physical or emotional stress, severe infection, hormonal changes, nutritional deficiencies, thyroid disease, or sudden weight loss. Fortunately, this type of hair loss is reversible once the underlying medical condition is addressed, allowing for new hair growth and restoration of healthy hair follicles.
- Triangular Alopecia

Triangular Alopecia, also known as temporal triangular alopecia, is a localized, non-progressive form of alopecia. It often begins in early childhood but can appear later. It manifests as patchy hair loss or thinning hair in triangular or oval areas around the temples.
The exact cause is unknown, but the hair follicles in affected areas are typically miniaturized, producing fine vellus hairs rather than terminal ones. This condition can be treated through medical therapy or hair transplantation if the hair does not grow naturally.
- Loose-Anagen Syndrome

Loose Anagen Syndrome typically appears in children and affects the anagen phase of the hair growth cycle. The hair shafts are loosely anchored to the hair follicles, allowing hair to be pulled out painlessly. This condition is more common in girls with light-colored hair and usually resolves over time as the hair follicles strengthen and grow hair normally again.
- Traction Alopecia

Traction Alopecia occurs due to chronic tension or pulling on the hair, often from tight hairstyles, braids, or the use of hair extensions. It commonly appears along the frontal hairline, resulting in patchy hair loss and, over time, scarring alopecia if not corrected.
Men who wear real hair wigs or synthetic wigs attached to existing hair may also experience traction alopecia, especially if worn for prolonged periods. If the pulling continues, this can lead to permanent hair loss or frontal fibrosing alopecia, a related cicatricial alopecia form.
- Trichotillomania
Trichotillomania is a mental health disorder involving compulsive hair pulling from the scalp, eyebrows, or other body hair regions. It is classified within obsessive-compulsive disorders rather than dermatological ones.
Over time, this repetitive behavior can lead to bald spots, scalp inflammation, and cicatricial alopecia in severe cases. Because it is a behavioral autoimmune-like condition associated with anxiety, effective management requires psychological assessment and therapy.
Persistent trichotillomania can destroy hair follicles and cause permanent scarring, leading to irreversible hair loss if left untreated.

- Scarring Alopecia

- Scarring alopecia, also called cicatricial alopecia, represents around 3% of all alopecia types and is responsible for permanent hair loss due to irreversible destruction of hair follicles.This group includes conditions where inflammation or autoimmune disease destroys the hair follicle stem cells, replacing them with fibrous tissue. Once destroyed, hair cannot grow back, leading to permanent bald spots or complete baldness in affected areas.
Primary vs. Secondary Scarring Alopecia
- Primary scarring alopecia occurs when inflammation directly targets the hair follicle, as seen in conditions like frontal fibrosing alopecia or central centrifugal cicatricial alopecia (CCCA).
- Secondary scarring alopecia results from external trauma, such as burns, radiation, or severe infection, where healthy hair follicles are destroyed as a side effect of injury.
Long-term traction alopecia and trichotillomania can also evolve into scarring alopecia if mechanical stress continues for years, resulting in permanent hair loss and visible bald spots.
Diagnosis of Alopecia
Determining what type of alopecia a person has is essential for choosing the right treatment options and predicting whether hair regrowth is possible. Because there are many alopecia types, each with unique characteristics, diagnosis must be performed by a qualified dermatologist or hair specialist.
During a physical examination, the doctor evaluates the scalp and hair density — whether it is diffuse, patchy, or follows a specific pattern baldness typical of androgenic alopecia.
They may also investigate the patient’s medical history, checking for autoimmune disorders, thyroid disease, hormonal imbalances, nutritional deficiencies, or mental health conditions that could contribute to hair loss.
In some severe cases, diagnostic tools such as scalp biopsy, trichoscopy, or blood tests may be required to assess immune system activity or rule out cicatricial alopecia (scarring alopecia). Identifying nail pitting, a common symptom of alopecia areata, can also help confirm diagnosis.
Treatment Options for Hair Growth and Alopecia Management
Treatment depends on the type of hair loss, its cause, and whether the condition is temporary or permanent. While not all treatments work for every patient, advances in medical therapy and hair restoration have significantly improved outcomes.
1. Medical Treatments
- Topical Treatments: Medications such as minoxidil help prolong the anagen phase and promote hair growth in both men and women with pattern baldness or female pattern hair loss.
- Oral Treatments: Finasteride or other anti-androgens can be prescribed for androgenic alopecia (especially in men).
- Corticosteroids: Topical or injected corticosteroids are used to suppress the immune system attacks that cause alopecia areata and promote hair regrowth in affected areas.
- Topical Immunotherapy: Used for resistant alopecia areata, this method stimulates a mild allergic reaction on the scalp to restart hair follicle activity.
2. Regenerative Therapies
- Low-Level Laser Therapy (LLLT): Utilizing an expert laser therapy hair loss treatment through ultraviolet light or laser stimulation improves cellular metabolism and strengthens the remaining hair shafts.
3. Surgical Options
For permanent hair loss cases, especially scarring alopecia or advanced pattern baldness, hair transplantation may be the only way to restore natural density. At Anastasakis Hair Clinic, advanced techniques like FUE (Follicular Unit Extraction) ensure natural-looking results and healthy regrowth from donor areas with strong hair follicles, or a traditional Follicular Unit Transplant (FUT) to harvest a strip of hair for maximum graft yield.
Every surgical hair transplant procedure is carefully planned based on the recipient area. For patients who have had unsuccessful procedures elsewhere, a hair transplant repair can effectively correct an unnatural hairline or poor density.
Conclusion: Timely Diagnosis and Personalized Treatment
If you are experiencing any form of hair loss or alopecia, timely diagnosis by a qualified hair specialist is essential. The earlier the specific type of alopecia is identified—whether alopecia areata, androgenic alopecia, scarring alopecia, or telogen effluvium—the higher the chances of achieving successful hair regrowth.
At the hair transplant clinic of Dr. Anastasakis, our team of experts provides comprehensive evaluation, including physical examination, medical history, and advanced diagnostic testing, to determine the underlying cause of your hair loss. We design a personalized treatment plan combining medical therapy, regenerative techniques, and surgical solutions to restore both hair density and patient confidence.
Early diagnosis, proper care, and the right treatment can make all the difference—helping you grow hair again, maintain healthy hair follicles, and prevent further hair loss for long-term results.
If you are experiencing hair loss, the only qualified professional to identify the underlying causes and design the optimal treatment strategy is a physician experienced and specialized in hair transplantation and hair loss therapies.




